Valentines Night Trail Run
Posted on January 12th, 2012 by Andries

Posted on January 12th, 2012 by Andries
Posted on January 11th, 2012 by Andries

Some questions and answers on the principles of skeletal muscle adaptations during training and exercise.
Posted on January 6th, 2012 by Andries

Most of the joints in our bodies, which allow us to move, are synovial joints. These joints rely on the diffusion of oxygen and nutrients within the joint fluid to nourish the cartilage. Effective diffusion of oxygen and nutrients within our joints requires movement of the joints. Unfortunately as a result of poor posture, chronic dis-use and acute injuries, joints tend to become ‘fixated’ and lose their ability to move correctly and sufficiently. Reduced movement will decrease the oxygen and nutrient supply within a joint and predispose a joint to inflammation and degeneration.

Scientific research specifically aimed at studying degenerative changes as a result of joint fixation (hypomobility) show that the process and extent of degeneration is directly affected by the length of joint hypomobility. Symptoms are numerous but includes pain and stiffness among others. Fortunately Chiropractic Care can assess and correct these affected joints in most people and subsequently promote joint health!http://www.sandtonchiropractic.com The research article discussed above can be read here.
Posted on January 5th, 2012 by Andries

Welcome back everyone. 2012 is here and exciting times await us! Just to get you all motivated and moving, here’s a couple of reasons why you should be physically active:
Optimism has been associated with enhanced inspiration, perseverance, and performance. Physical activity could influence optimism through mastery of experiences, through its impact on reducing anxiety and lowering levels of depression, and enhances self-efficacy. Therefore the hypothesis stated that active individuals are more optimistic and less pessimistic than their less active counterparts.
It’s the time where you become one with the environment and just loose yourself and generate energy from it. It’s been found that when individuals don’t participate in any physical activities, they become lazy, and get this feeling of constant tiredness. But when you exercise, you feel energetic, relaxed, and motivated. Therefore being more physically self-efficient and decreasing the state of anxiety. Pessimistic people on the other hand are found to be more inactive due to increased fear of potential failure, therefore leading to higher levels of depression because of their low physical self-efficacy.
Being positive in life and being optimistic depends on every individual him/herself. It is all an indication of how strong you are psychologically, emotionally and physically. But without any physical activity, you feel lethargic and depressed. Optimism gives you control over your environment and attributes to a more positive outlook upon exercise and life itself.
Kavussanu, M. & McAuley, E. (1995). Exercise and optimism: are highly active individuals more optimistic? Journal of Sport and Exercise Psychology, 17, 246-258.
Hope you all have a great year and looking forward to sharing more knowledge and experiences with all of you during 2012.
If you have any queries or questions or need more info on anything that interests you, leave a comment and I’ll add it to InSession.
STAY INJURY FREE BY BEING ACTIVE
Posted on December 20th, 2011 by Andries Lodder

Claims by manufacturers:
The purpose of the present study was to investigate how MBT changes the gait pattern and muscle activation.
Research Findings:
Romkes, J., Rudmann, C. & Brunner, R. (2006). Changes in gait and EMG when walking with the masai barefoot technique. Clinical Biomechanics. 21 (1): 75 – 81.
Claims by manufacturers:
The aim of this study was to systematically assess the effect of the MBT shoe on plantar pressure.
Research Findings:
Stewart, L., Gibson, J. N. & Thomson, C. E. (2007). In-shoe pressure distribution in “unstable” (MBT) shoes and flat-bottomed training shoes: a comparative study. Gait Posture. 25 (4): 648 – 651.
When standing on once toes, or contacting of extrinsic plantar flexor muscles, the calcaneus raises and thereby shifting the distribution of body weight from the heel to the forefoot, or in this case over the metatarsal heads. Due to the hyperextension of the metatarsalphalangeal joints, the plantar fascia stretches and creates an increase angle of the medial longitudinal arch. Therefore strengthening the midfoot and hindfoot. With this occurring, the contraction of the intrinsic muscles provides additional reinforcement to the arch (Newmann, 2002, pp. 506).
Abnormal pronation mimics the effect of a foot with pes planus, or flat foot. This puts a limitation on the amount of height of a rise up on tiptoes. Accompanied with pes planus, comes a poorly supported medial longitudinal arch. Due to the lack of hyperextension of the metatarsalphalangeal joint, creates an unstable midfoot and forefoot due to the distribution of body weight being uneven over a area with little support were the arch remains flattened (Newmann, 2002, pp. 506).
Posted on December 18th, 2011 by Andries Lodder
The aims of stretching are to gently lengthen muscles before and after any form of exercise, and to improve tissue elasticity / flexibility. If done correctly, stretching will help prevent injuries and increase athletic performance.
The following key points should be remembered whilst stretching:

Sitting on the floor with the soles of the feet together, place your hands either around your ankles or lower legs. Keeping your back straight gently open out the knees towards the floor, applying a steady stretch onto your adductor / inner thigh muscles. The elbows can be pressed against the inner knee to increase the stretch. Avoid pulling up on your feet during the stretch.

Standing one foot in front of the other, feet comfortably apart, both feet facing forward, front leg bent (knee over ankle joint), back leg straight, back straight.Press the heel of the back leg into the floor until a stretch is felt in the calf muscle in the back of the lower leg. If no stretch is felt, slide the heel slowly backwards, keeping the foot on the floor.For improved stability and a greater stretch, push against a wall.

Sit up with your left leg out straight, and your right leg crossed over at about the knee joint, placing the foot flat on the floor. Using your right arm, pull the bent left leg slowly across, until you feel the stretch in the right buttock region. Simply reverse both leg and arm to do the other side.

Lie on your back, bending one leg keeping that foot on the floor, to prevent you lifting your buttocks during the stretch. Raise your other leg, holding it either side of your knee joint, to gradually pull the leg towards you. You should feel the hamstring muscle stretching at the back of this leg. Concentrate on keeping your buttocks on the floor, and keeping the stretched leg as straight as possible.

Lie on your back, with your legs bent up towards you. Keeping your upper back firmly on the floor, gently lower your knees to one side, hold for about 20 seconds, then repeat on the other side. Allow your lower back to rotate naturally to the side, however if any pain is felt avoid this stretch.

Whilst on all fours, look down towards the floor, then push your shoulders as high as they can go. This stretch is often called a cat stretch, due to the motion made. Aim to hold in the stretched up position for 10 seconds before repeating.

Place one leg forward with your knee above your toe, and the other stretched back with that knee touching the floor. Your hands can be placed on the front leg or floor to aid balance. Slowly push the pelvis forward until you feel the stretch in the upper thigh / hip flexor muscle of the rear leg.
Posted on December 18th, 2011 by Andries Lodder
While studying Exercise Physiology at Wits, we did this research project. I thought I’d share it with you all.

The purpose of this study was to investigate what effects spinning have on sweat rate under certain environmental conditions and to investigate what other variables contribute to sweat rate changes.
Sixteen healthy regular spinners took part in a 45-minute spinning class on three separate days. Pre and post nude body weight, amount of water consumed, heart rate and ratings of perceived exertion (RPE), dry- (TDB) and wet-bulb temperatures (TWB) and were measured throughout the duration of the spinning class.
A linear relationship between sweat rate and RPE and weight loss were correlated. Therefore an increase in RPE caused an increase in sweat rate, which lead to an increase in body weight loss post spinning (R2 = 0.3569; R2 = 0.3693; respectively; p < 0.05). No significant difference was observed for TDB, TWBand relative humidity between each of the three days (p = 0.3532; p = 0.4933; and p = 0.4580; respectively; p > 0.05).
During a high intensity spinning class, the greater the RPE, the higher the sweat rate, and the greater the post spinning body weight loss. Additional studies need to be done under different ambient conditions, to determine whether a change in those conditions would have an effect on sweat rate.
sweat rate; spinning class; fluid replacement
Spinning has hit the world by storm. More and more people, including cyclist, take part in spinning classes due to everyday lives getting busier and national roads more dangerous to cycle on, leaving less time for exercise in the outdoors. Spinning, being an indoor event in a controlled environment, simulate a high intensity training session, but being indoors, the effects on and of the human body will be different than it would be outdoors. Therefore the question arose of what effects occur on the body during a spinning class, what effect does it have on sweat rate under certain environmental conditions, and therefore to investigate what other variables contribute to sweat rate changes.
Sixteen (3 males and 13 females) healthy regular spinners, aged 31 ± 10 years (mean ± SD) and mass 67.2 ± 10.5 kg, volunteered to participate in this study. The experimental protocol was approved by the University of the Witwatersrand Committee for Research on Human Subjects (M020804) and all subjects gave written consent before participation.
Volunteers were recruited from Planet Fitness Spinning Studio, Wanderers, Johannesburg. The same instructor conducted all three spinning classes at similar intensities on three separate days at 5pm during the month of October 2006, in an enclosed air-conditioned environment. Before the start of the spinning class they completed a questionnaire that assessed spinning history, fitness levels and daily hydration and health status.
Before and after each class, nude body weight was measured using an electronic scale (SECA Alpha scale, Model 770, Germany). The spinners were asked to empty their bladders before measuring their pre-spinning weight and to towel off any excess sweat before measuring their post-spinning weight. The amount of water they consumed during the class was determined by measuring the amount of water in their bottles before the class, and the amount remaining at the end of the spinning class.
All participants wore Polar Heart Rate Monitors (FS3C model; Polar Electro, Kempele, Finland) for the duration of the class. Heart rate (HR) was recorded every 5 minutes from the start of the spinning class. Rate of perceived exertion (RPE), an indicator of how hard they felt they were working, was determined every 5 minutes using the 10-point Borg Rating scale (Borg, 1970).
Dry-bulb temperature (TDB) and wet-bulb temperature (TWB) were measured every 10 minutes using a Whirling Psychrometer (Haden, England). Relative humidity was calculated using a psychrometric chart.
Data are shown as mean ± standard deviation unless otherwise stated. A Spearman’s correlation was used to determine the relationship between RPE and sweat rate and amount drunk. A Pearson’s correlation was used to determine the relationship between sweat rate and percentage of heart rate maximum, heart rate maximum, weight loss, amount drunk and average heart rate, as well as between average heart rate and amount drunk. A paired t-test was used to analyze for differences in body weight before and after the spinning classes. A one-way ANOVA test was used to determine the relationship between TDB, TWB and relative humidity. All statistical analysis was performed using GraphPad InStat version 3.00 for Windows 95, GraphPad Software, San Diego. California USA. Statistical significance was set at P< 0.05.
Subject characteristics, significant results, physiological responses and ambient environmental conditions during the spinning class of the 16 spinners are represented in Table 1 below.
Table 1 – Table showing weight fluctuations, water consumption, and sweat rate during a spin class in the 16 spinners, as well as the ambient environmental conditions (mean and SD).
| Age (yrs) | Body Weight before (kg) | Body Weight after (kg) | Body Weight loss (kg) | Amount drunk (l) | Sweat rate (l/hr) | TDB* (°C) | TWB** (°C) | Relative Humidity (%) | |
| Mean | 31 | 65.3 | 64.7 | 0.4 | 0.405 | 1.1 | 20.1 | 14.6 | 57.7 |
| SD | 10 | 10.5 | 10.6 | 0.3 | 0.263 | 0.3 | 0.6 | 0.2 | 2.5 |
| *TDB: Mean Dry-bulb temperature for 3 the days | |||||||||
| *TWB: Mean Wet-bulb temperature for the 3 days |
We observed a decrease in overall body mass (0.4 ± 0.3 kg) for all participants, which were only statistically significant, but not biologically significant (p = 0.0003; r = 0.9996; 95% confidence interval of the difference: 0.2083 – 0.5542, respectively).
We observed a significant relationship between RPE and sweat rate (y = 2.4759x + 2.692; R2= 0.3569; p 0.05).

Figure 1 – Linear relationship between RPE and sweat rate (litres/hr)
We found a significant relationship between sweat rate (litres/hr) and weight loss (kg) (y = 0.5923x + 0.2942; R2= 0.3693; p 0.05).

Figure 2 – Linear relationship between sweat rate (litres/hr) and weight loss (kg)
We observed no significant difference for TDB, TWB and relative humidity between each of the three days (p = 0.3532, F = 1.136; p = 0.4933, F = 0.7500; and p = 0.4580, F = 0.8339; respectively; p > 0.05). Table 2 below represents the mean and standard deviation differences in TDB, TWBand relative humidity during the three separate days of spinning.
Table 2 – Dry-bulb temperature (TDB), Wet-bulb temperature (TWB) and relative humidity (%) for the three days of spinning| TDB* (°C) | TWB** (°C) | Relative Humidity (%) | |
| Mean ± SD | Mean ± SD | Mean ± SD | |
| Day 1 | 20.4 ± 0.9 | 14.8 ± 0.4 | 57.0 ± 4.5 |
| Day 2 | 19.4 ± 1.1 | 14.4 ± 0.5 | 60.4 ± 7.1 |
| Day 3 | 20.4 ± 1.5 | 14.6 ± 0.5 | 55.6 ± 6.3 |
| *TDB: Dry-bulb temperature | *TWB: Wet-bulb temperature |
The aim of this study was to determine the effects of a high intensity spinning class on sweat rate. Therefore to determine how much fluid needs to be consumed to prevent either hyperhydration or hypohydration.
We found that sweat rate has a good linear relationship between RPE as well as weight loss during a 45 minute spinning class. As intensity increases, and therefore an increase in RPE, sweat rate will increase, as well as indirectly have an effect on weight loss.
All these variables (sweat rate, RPE and weight loss) are interrelated.
The effects of a high intensity spinning class are on average a high RPE rating, an increased sweat rate, and a decrease in body weight. During a spinning class, or any physical exercise, hydration is a very important factor contributing towards body temperature regulation, exercise performance and the prevention of the development of heat injury (Convertino et al, 2005).
During the 45 minute spinning class, the difference between the body weight before and after the spinning class, decreased. This could be affected by the amount of fluid consumed or at what intensity the participant was working at. Therefore if the spinner consumes too much fluid (hyperhydration), the smaller the difference in body weight before and after. The same goes for if the spinner consumes too little fluid (hypohydration), the difference between weight before and weight after will be much greater.
An increase in RPE showed a linear correlation to an increase in sweat rate. This was expected, due to the higher the intensity a person works at, the more heat that person is going to produce, therefore to regulate their body temperature and keep it constant, they will increase their sweat rate to eliminate excess heat from the body. No correlation was observed between RPE and amount of water consumed. An increase in RPE will have an effect on thirst, but it is up to the person self to make a conscious decision to consume the water, therefore its very subject specific.
Ambient temperatures for all three days were very similar, no significant differences between the three days. (Mean ± SD; TDB = 20.1 ± 0.6 °C; TWB = 14.6 ± 0.2 °C; and relative humidity = 57.7 ± 2.5 %). These contribute to a controlled environment and increase the validity and reliability of results obtained for these conditions.
Looking at table 1, if you take the means, for a person that weighs approximately 65.3 kg, and drinks only 405 ml water during the 45 minute spinning class, will loose on average 0.4 kg body weight, mostly water, and will have a sweat rate of 1.1 litres/hr.
In the condition of our present study, it has shown that participating in a high intensity spinning class, body weight will be decreased if an insufficient amount of water was consumed. Another important factor that effects body weight loss, is the intensity that a person works at, therefore working at a higher RPE, sweat rate will be increased, and therefore increase body weight loss. These variables all-dependent on the amount of water intake, either hypohydration occurs, which will increase post body weight loss, or hyperhydration, which will decrease post body weight or even increase post spinning body weight. Additional studies need to be done under different ambient conditions, to determine whether a change in those conditions would have an effect on sweat rate.
Posted on December 5th, 2011 by Andries Lodder
 Your problem probably originates from cycling more than swimming because the pain is worse after a hard bike session. Pain in the Achilles usually indicates a problem in pedaling technique, where the saddle is set too high and forces the cyclist to point the toes excessively to reach the bottom of the pedal swing. Having your cleats set too far forward, or otherwise pedaling with your toes can also cause it. The farther forward the contact between the foot and the pedal, the greater the stress on the Achilles tendons. The main reason why you’re feeling it mostly during swimming is because your feet are plantar flexed (toes pointed down) during swimming, causing the calf muscles to be under constant contraction and under tension the whole time.
As a guideline, more information or an assessment is needed, as many contributing factors still need to be taken into account for a more accurate diagnosis, but these are my recommendations:
Your problem probably originates from cycling more than swimming because the pain is worse after a hard bike session. Pain in the Achilles usually indicates a problem in pedaling technique, where the saddle is set too high and forces the cyclist to point the toes excessively to reach the bottom of the pedal swing. Having your cleats set too far forward, or otherwise pedaling with your toes can also cause it. The farther forward the contact between the foot and the pedal, the greater the stress on the Achilles tendons. The main reason why you’re feeling it mostly during swimming is because your feet are plantar flexed (toes pointed down) during swimming, causing the calf muscles to be under constant contraction and under tension the whole time.
As a guideline, more information or an assessment is needed, as many contributing factors still need to be taken into account for a more accurate diagnosis, but these are my recommendations:
Posted on December 5th, 2011 by Andries Lodder

When it comes to making changes in your physique, you must get clear on what you want, and be honest with yourself from the beginning. Perfection is not required, but there is a great balance between work done in the kitchen, and in the gym. Lets make your goal a reality.
When it comes to diet, there is no perfect meal, however, it comes down to calories in vs. calories out. It’s as easy as that!
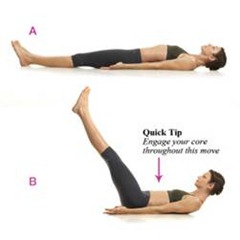
The abdominals are composed of four main muscles: The Rectus Abdominis, External Oblique, Internal Oblique, and Transversus Abdominis. Each muscle has a role in the stabilization of a strong core, and the approval of all on the beach. Implement a routine that hits each one of these muscle groups to an equal degree for a intense workout:








Cool-down: 50 trunk twists – 2 sets, 25 full sit-ups
Other exercises to add variety: Balance ball knee crunch, Roman chair raises.
This is a fairly advanced routine, and beginners should use caution and start out using one set of each exercise. Use a stopwatch and see how long it takes you to complete the workout and try improve on it every time.
This is a very manageable strategy to get that body we all die to show off at the beach. Now stop reading and start planning.
http://pure-nt.co.za/blog/beach-abs/Posted on November 10th, 2011 by Andries Lodder
 With summer on our doorstep and days getting longer and warmer, many people are taking to the outdoors to find their fitness fix. And, what better way to enjoy this country’s spectacular natural areas and climate than through mountain biking or cycling. Many have set the annual 94.7 Cycle Challenge as their goal, and with the event around the corner beginners and experienced cyclists alike have been taking to streets and off-road trails in preparation.
With summer on our doorstep and days getting longer and warmer, many people are taking to the outdoors to find their fitness fix. And, what better way to enjoy this country’s spectacular natural areas and climate than through mountain biking or cycling. Many have set the annual 94.7 Cycle Challenge as their goal, and with the event around the corner beginners and experienced cyclists alike have been taking to streets and off-road trails in preparation.
Aside from knowing where the best spots are to enjoy a post-cycle breakfast, what else do cycling enthusiasts really need to know? Fitness and preparation for any sporting activity include understanding the associated risks – making this an opportune time to delve into common cycling injuries.
There will always be traumatic injuries that result from falls and other unplanned adverse events, the effect of which a physiotherapist will do their best to mitigate, to encourage healing. However what many physiotherapists deal with is the effect on the body of the repetitive motion and rhythm of cycling, which can cause what is called a repetitive strain injury due to incorrect biomechanics.
These postural problems can be minimized far in advance of commencing cycling by spending a little extra money on ensuring that a bicycle is set up correctly for an individual’s unique physiology – by a professional.
Something as simple as making sure your saddle is at the correct height and that your cleats are in the right position – and not rotated – can go a long way towards preventing much future discomfort and injury.
That said, the cycling position is not a natural one and following training in this position for extended periods of time many cyclists develop weakness of their hip extensors (which move hips backwards), their abductors (which move hips outward), lateral rotators (which turn the hips out to the side) and over activity of the hip flexors (which move hips forward), the adductors (which move hips inwards) and the medial rotators (which turn hips inward).
It is also very common for cyclists to have very tight calf muscles, which affects range of movement at the ankle making cyclists more prone to injury in that area. Remember to always stretch hip flexors, adductors, medial rotators as well as the calf muscles adequately before and after training.
It’s very important for cyclists to strengthen their hip extensors, abductors and lateral rotators. A very good way to do that is to start cross training i.e. exercising off the bike to target these muscle groups through other forms of exercise. It has also been shown that cyclists have a lower bone density -especially in the lumbar spine and hips – due to excessive calcium loss through sweating and all the hours spent on the bike. As cycling is a non-weight bearing activity it doesn’t promote an increase in bone density, but cross training – particularly doing weight-bearing exercises – will ensure bone density remains optimal.