BRUXISM
Posted on May 5th, 2016 by Andries Lodder
THE DISORDER ASSOCIATED WITH GRINDING AND CLENCHING OF YOUR TEETH
By Dr. Ashana Harryparsad, BDS (WITS), PDD (UWC), MChD (UP), Specialist Prosthodontist, Netcare Waterfall City Hospital.
Grinding or clenching of your teeth is medically diagnosed as bruxism, and can occur while asleep or awake. Few entities in the dental fraternity are as perplexing as bruxism. Its prevalence in the general population is 10%.
Bruxism has reached the extremes of diagnosis; from being the ‘most destructive process of the oral cavity’ to ‘nothing more than a manifestation of a benign routine activity’. Bruxism can be classified as primary or secondary.
Primary bruxism presents as clenching or grinding of the maxillary and mandibular teeth either during sleep or awake periods. It is one of the most significant disorders related to the oral cavity as several related clinical symptoms occur in the temporomandibular joint (TMJ), periodontium (area around a tooth), masticatory muscles (chewing muscles) and to the teeth.
During sleep, it is usually identified by a grinding sound and is frequently noticed by a bed partner. Sleep bruxism is related with other sleep disorders such as snoring and sleep apnoea. As a consequence of the grinding, a specific type of tooth wear is produced which manifests as wear facets. This is the more common variant of sleep bruxism, relating to 52.5% of sleep bruxers.
A less common type of sleep bruxism is when patients clench. It is far less damaging to the dentition, however causes fatigue within the facial muscles and muscular pain when the patient wakes. This type of bruxism occurs in 11.4% of sleep bruxers.
The final type of sleep bruxism occurring in 36.1% of sleep bruxers is termed mixed bruxism. It comprises a combination of the above-mentioned types of sleep bruxism.
While awake, the most common type of bruxism is clenching, and it arises primarily when concentrating or stressed, and patients are often surprised that they are clenching. Grinding while awake is less common and also less destructive, except in those suffering from neurologic disorders.
Secondary, pharmacologic or iatrogenic bruxism are common terms for a condition seen in patients using neuroleptics or antidepressants and is a side effect of drug therapy.
Scientific literature reveals that the diagnosis of the existence and severity of bruxism is a highly complex task, given that the exact aetiology remains unknown. The preferable methods, electromyography and polysomnography, are not suitable for routine use, therefore the use of clinical assessment coupled with a form of questionnaire highlighting key aspects of bruxism is the preferred method for diagnosis.
Questionnaires typically are based on a series of common questions, including the following:
- Do you wake up with pain/tenderness of your jaw muscles?
- Do you ever have tooth or gum pain upon awakening?
- During the day, do you tend to clench your teeth?
- Do you ever grind your teeth during the daytime?
- Does your partner notice that you grind your teeth loudly at night?
CAUSES OF BRUXISM
In the past, the dental associated causes of bruxism included abnormal bite (malocclusion) or missing or maligned teeth. However, recent scientific literature has shown no correlation between occlusion (i.e. how your teeth come together) and bruxism. These studies show a stronger association with disorders of the central nervous system and behavioural involvement.
Stress and anxiety have been strongly associated with bruxism. In some patients, the condition may worsen or develop during periods of severe stress and then disappear once the stressful period has passed.
Obstructive sleep apnoea has also been associated with bruxism, however the correlation between the two is not fully understood.
Other medical conditions which bruxism may manifest as a symptom include Huntington’s disease, Parkinson’s disease, Basal ganglia infarction and post-traumatic stress disorder (PTSD).
Specific medication, such as antipsychotic and antidepressant medication can also cause or perpetuate bruxism. Lifestyleassociated activities such as regular alcohol consumption, smoking and the use of recreational drugs (i.e. cocaine and ecstasy) have also been associated with an increase in bruxism.
SIGNS AND SYMPTOMS
Sleep-associated bruxism often goes undetected by the patient, until it becomes symptomatic. The most commonly associated symptoms include a dull constant headache, or sore jaw/muscles of the jaw when you awake. Most sleep bruxers become aware of their problem from their loved ones, who hear them grinding at night.
To summarise, the signs and symptoms of bruxism may include:
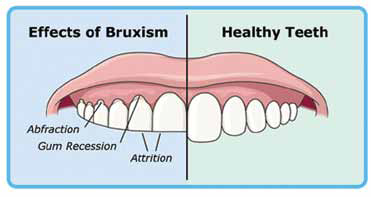
- Severely worn teeth. Severe cases of bruxism can result in short teeth (stumps) which can result in aggravation of existing temporomandibular disorders, loss of teeth or increased tooth pain and sensitivity.
- Fractured teeth or fillings;
- Difficulty in mouth opening;
- Facial muscle pain (Facial myalgia);
- Earache;
- Headaches, originating in the “temples”;
- Tightness and stiffness in the shoulders;
- Pain and stiffness of the temporomandibular joint – signs may include “clicking” or crepitus of the joint when you open and close your mouth;
- Sleep disruption / poor sleep quality.
RISK FACTORS
Factors which may increase your risk of bruxism include:
- Stress
- Age: Grinding or clenching is common in young children, but this usually subsides as they get older.
- Personality type: competitive, aggressive or hyperactive personality types have been associated with an increase in bruxism.
- Stimulating substances: tobacco, drinking caffeinated beverages or alcohol and recreational drugs.
WHEN TO SEE A DENTAL PROFESSIONAL
You should see a dental professional, such as a Prosthodontist, who has been trained in treating bruxism, when you present with one or more of the following:
- Your teeth are showing signs of wear, damage or sensitivity;
- You have pain in your jaw, face or ear;
- Your partner complains that you make a grinding sound in your sleep.

If you do not present with the above symptoms, but suspect you may be grinding/clenching your teeth, please consult a dental professional. They will perform the appropriate examination to determine whether you are a “bruxer” and formulate an appropriate treatment plan for the underlying cause.
POSSIBLE TREATMENT OPTIONS
Due to the uncertainty of the true aetiology of bruxism, treatment of it can be complicated and difficult. Treatment is therefore directed to treating/reducing the symptoms.
Treatment options for the teeth depend on the severity of damage to the teeth. Dental treatment ranges from a mouth guard/splint to a complete rehabilitation with crowns, bridges, implants or dentures.
Identification and treatment of the possible underlying cause/s will aid in reducing the symptoms.
Reduction of stress or anxiety via lifestyle changes or medication may be needed. In cases with severe muscle pain or temporomandibular disorders, treatment is done in conjunction with a physiotherapist. Sleep disorderassociated bruxism will require appropriate diagnosis and treatment of the disorder.
Other basic tips to assist with alleviation of your symptoms may include:
- Reduction of caffeine intake;
- Reducing/avoiding alcohol consumption;
- Avoiding chewing gum or hard foods to allow your muscles of mastication to relax;
- Warm compress treatment, including placement of a warm compress to the muscles of the jaw to aid in pain relief.
In severe cases of bruxism, which do not respond to other treatment, botulinum toxin A (‘Botox’) injections may help.
Regular dental visits may assist in the early detection of bruxism, thereby preventing severe complications associated with this disorder.
References:
- Paesani DA. Bruxism theory and practice. Quintessence publishing Co LTD. 2010
- Behr M, Hahnel S, Faltermeier A, Bürgers R, Kolbeck C, Handel G, Proff P. The two main theories on dental bruxism. Annals of anatomy. 2012;194:216-219
- Diracoglu D, Alptekin K, Cifter ED, Guclu B, Karan A, Aksoy C. Relationship between maximal bite force and tooth wear in bruxist and non-bruxist individuals. Arc Oral Bio. 2011;1569-1575
- Clark GT, Rugh JD, Handelman SL. Nocturnal masseter muscle activity and urinary catecholamine levels in bruxers. J Dent Res. 1980;59: 1571-1576
- Manfredini D, Bucci MB, Sabbatini VB, Lobbezoo F. Bruxism: Overview of current knowledge and suggestions for dental implants planning.
- J Craniomand Prac. 2011; 29: 304-312.
- Dao TTT, Lavigne GJ. Oral Splints: The crutches for temporomandibular disorders and bruxism? Crit Rev Oral Biol Med. 1998; 9(3): 345-361
- MedlinePlus : “Bruxism”
- Mayo Clinic: “Bruxism/Teeth Grinding.”
- WebMD: “An Overview of Teeth Grinding (Bruxism)”
For more info please contact Dr. Ashana Harryparsad at prostho@waterfallhealth.co.za
Original article post in Waterfall News Issue 3, 2016.
Tweet